 Chief Medical Officer, Professor Chris Whitty and Chief Scientific Adviser, Sir Patrick Vallance give a Coronavirus Data Briefing in 10 Downing Street on September 21st. Picture by Pippa Fowles / No 10 Downing Street.
Chief Medical Officer, Professor Chris Whitty and Chief Scientific Adviser, Sir Patrick Vallance give a Coronavirus Data Briefing in 10 Downing Street on September 21st. Picture by Pippa Fowles / No 10 Downing Street.
How a novel virus met a partly-immune population
In Spring 2020 a novel coronavirus swept across the world: novel, but related to other viruses. In the UK, unknown at the time, around 50% of the population were already immune. The evidence for this is unequivocal and arose due to prior infection by common cold-causing coronaviruses (of which four are endemic). This prior immunity has been confirmed around the world by top cellular immunologists. There is even a very recent paper from Public Health England on the topic of prior immunity and a wealth of other evidence from studies on memory T-cells, studies on household transmission and on antibodies.
Because of the extent of the prior immunity, and as a result of heterogeneity of contacts, once only a low percentage of the population, perhaps as low as 10-20% had been infected, “herd immunity” was established. This is why daily deaths, which were rising exponentially, turned abruptly and began to fall, uninterrupted by street protests, the return to work, the reopening of pubs and crowded beaches during the summer. (See this explainer by the data scientist Joel Smalley.)
Immunity to ordinary respiratory viruses occurs mainly through T-cells which ‘take a picture of the invader’ at a molecular level, ‘reproduce’ it on certain immune cells and essentially ‘never forget a face’. This T-cell immunity is robust and durable. Those exposed to the highly related SARS virus in 2003 still have this immunity 17 years later. In relation to SARS-CoV-2, the pattern of immunity to date is identical and after around 800 million infections across the world, there is no convincing evidence for significant levels of re-infection. Not only are those who’ve been infected and have now recovered immune (they cannot get ill again with the same virus), but importantly they do not participate in transmission. (See my article on what SAGE got wrong for Lockdown Sceptics.) Furthermore, because the immune response is diverse, a proportion of them will also be immune to novel but similar viruses in the future.
In Spring, however, this virus did kill or hasten the end for approximately 40,000 vulnerable people, who were mostly old (median age 83, which is longer than that cohort’s life expectancy when born) and many of whom had multiple other medical conditions. There were some rare and very unfortunate younger people who also died, but age is clearly the strongest risk factor.
But due to extraordinary errors in modelling created by unaccountable academics at Imperial College, the country was told to expect over a half a million deaths. Three Nobel prize-winning scientists wrote to that modelling team in February correcting their errors. This was done confidentially. This expert, third-party estimate was remarkably accurate – it predicted that there would be a total of 40k deaths from COVID-19. I believe this is in fact correct and is what has happened. While I have no proficiency in modelling, I can distinguish predictions that are biological plausible from those which are literally incredible. When inputs to a model are wrong or missing, their outputs cannot be trusted. The Imperial model made the extreme assumption that there was zero prior immunity in the population or social contact heterogeneity.
It is now appreciated that this virus is less of a threat to those under 70 than seasonal flu, even with a flu vaccine, which routinely provides <50% effectiveness and usually much less.
The ease with which humans develop immunity to this virus is striking. Incidentally, it is this immune adeptness which has probably played an important role in why, against prior pessimism, many vaccines for SARS-CoV-2 have apparently ‘worked’ (though there is much to criticise about how efficacy has been defined, because a reduction in the propensity to become PCR positive has not previously been regarded as a leading indicator of the degree to which a vaccine will protect a population against severe illness).
Available evidence suggests that herd immunity at a national level (in England) was attained as early as May. (Joel Smalley again.) There have been no alternative explanations promulgated for the force which bore down on infections and deaths during the largely unmitigated spreading of the virus early in Spring. As an example of evidence that we are at herd immunity, London is relatively peaceful in relation to the virus now, having been the national epicentre in Spring, with hundreds of deaths daily in the capital.
Government actions have been nothing but peculiar from the very beginning
In any other year, that would be the end of the tale. Neither the existence of prior immunity nor that herd immunity can be readily reached without us noticing are new.
What was new was the belief that forcing citizens to run and hide from a respiratory virus with greater contagiousness than ‘flu was other than a fool’s errand. Acts of Parliament giving the executive a degree of power more suited to a war, and with it, a budget 10 times larger than any previous such emergency, were also deemed necessary, none of these being justified by the situation or by science. (See Jonathan Sumption make this point.)
We were invited to “Save the NHS” by the expedient of not attending hospitals or seeing our doctors: soon both were heavily restricted and have remained so ever since. Most corrosively, broadcasters were and still are heavily constrained from free expression by innocent-sounding Ofcom guidelines.
I am of the view that the effect of these guidelines approximates censorship. When scientific debate is stifled, people die. Science requires the airing of opinions and debate to allow the evolution of ideas. Censorship has meant that nothing has been learnt, no model adjusted and errors compounded.
The Government was told to expect a ‘second wave’, and a huge one at that. This was mystifying. Virus don’t do waves and no reason to expect an exception on a truly unprecedented scale has ever been forthcoming. I hasten to distinguish what I have termed a secondary ripple from what SAGE means by a ‘second wave’.
The secondary ripple term recognises that not everyone will have been infected by mid-summer. As an important aside, I’ve invited many to consider how long it takes for an influenza epidemic, which we experience most years, to criss-cross the country before apparently burning out, only to occur the next year, because it’s one of the few respiratory viruses which mutates so quickly that, by the time a year has gone by, it’s sufficiently different from what our immune systems have seen before that it can wreak brief havoc upon us once again. The answer to that time question is variously given as three to four months.
I ask readers to consider how long might it be expected to take for a more contagious respiratory virus like SARS-CoV-2 to thoroughly criss-cross the country. It seems hard to credit that with taking longer than four months. We know the virus was in the UK at least by February 2020 (potentially earlier) and so by June it’s not at all unlikely that it had travelled almost everywhere. It has been argued that perhaps lockdown was very effective and so many people will still be susceptible, as SAGE claims. We know that is not correct. Lockdown was started far too late to repress the spread of the virus, as even Professor Whitty agreed in giving testimony to a parliamentary select committee in the summer. As he said, the lockdown began after the peak of infection – the outbreak was already in retreat by Mar 23rd.
Remember also that just because we were in ‘lockdown’ doesn’t mean much changed when it came to the transmission of the virus. Many people continued to go to work, other people still shopped almost every day, supply chains for all essential goods continued with few interruptions. Hospitals were open and, for the most part, extremely busy, as were care homes. The virus travelled along these routes and did not need to travel far, having reached every major urban centre before anyone even thought of locking us down or any other measures. When lockdown was lifted, there wasn’t the slightest alteration in the long, slow decline in the number of daily deaths. Personally, I don’t think there’s any evidence that the spring lockdown achieved anything in terms of saving lives from SARS-CoV-2, but there is evidence it contributed to some deaths, including deaths from non-COVID-19 causes. Reflecting back, months after, its main effect was to condition us to accept SAGE’s guidance as this was followed by the Government and echoed by media. This doesn’t mean locking people down is a sensible policy. The onus remains on its advocates to persuade us that it is, and I’m afraid they’ve not persuaded me.
So, no: there’s no good reason to think that large proportions of the nation were spared exposure to the virus as a result of the first lockdown. But it is true that some regions did experience less deaths in spring than others and while some are almost certainly due to more extensive prior immunity, others probably were incompletely exposed. That’s what I mean by secondary ripple: as transmission was increased by cooler weather, a limited amount of disease did reappear. But this was always going to be local, self-limiting and under no circumstances a public health emergency for a city, let alone a nation. This secondary ripple started at the beginning of September and was over by the end of October. Symptom-tracking data, NHS triage data and notified disease data all support that hypothesis. After this ripple, immunity levels in the underexposed pockets of the country have been topped up to herd immunity levels. From now on, COVID-19 outbreaks will be a feature of winter but will not be able to spread beyond small outbreaks.
No, what SAGE meant by a ‘second wave’ was a really big one, with twice as many deaths as in spring 2020. This is completely without precedent.
Planning for a ‘second wave’ might have led to its very creation
Viruses don’t do waves (beyond the secondary ripple concept as outlined above). I have repeatedly asked to see the trove of scientific papers used to predict a ‘second wave’ and to build a model to compute its likely size and timing. They have never been forthcoming. It’s almost as if there is no such foundational literature. I’m sure SAGE can put us right on this.
The post-WW1 “Spanish flu” appears to be all there is where it comes to evidence of waves. Most scholars accept that what most likely happened was that more than one infectious agent was involved. It was 102 years ago and no molecular biological techniques indicate multiple waves of a single agent then or anywhere else. In any case, that was influenza. There have been no examples of multiple waves since and the most recent novel coronavirus with any real spread (SARS) performed one wave each in each geographical region affected. Why a model with a ‘second wave’ in it was even built, I cannot guess. It seems completely illogical to me. Worse, as far as the public can discern, the model fails to account for the unequivocally demonstrated population prior immunity, to which must be added the recently-acquired immunity arising from the spring wave. This is why I’m reasserting what I’ve been argued for months – a ‘second wave’ cannot happen and must, perforce, not be happening as described
Despite the absence of any evidence for a ‘second wave’ – and the evidence of absence of waves for this class of respiratory virus – there was an across-the-board, multi-media platform campaign designed to plant the idea of a ‘second wave’ in the minds of everyone. This ran continually for many weeks. It was successful: a poll of GPs showed almost 86% of them stated that they expected a ‘second wave’ this winter.
As research for this piece, I sought the earliest mention of a ‘second wave’. Profs Heneghan and Jefferson, on Apr 30th, noted that we were being warned to expect a ‘second wave’ and that the PM had, on Apr 27th, warned of a ‘second wave’. The Professors cautioned anyone making confident predictions of a ‘second’ and ‘third wave’ that the historical record doesn’t provide support so to do.
I looked for mentions by the BBC of a ‘second wave’. The following report was on June 24th and at least two of the three scientists interviewed were SAGE members. The strange thing though is that SAGE minutes (brought into the public domain by Simon Dolan’s judicial review) early in the year made no mention of a sizeable ‘second wave’. Not one. On February 10th, there was a mention of multiple waves for post-WW1 flu. On Mar 3rd and 6th, there is mention of a single SARS-CoV-2 wave with most (95%) of the impact early on. What looks to be the final document, Mar 29th, still just refers to one wave. This is what history and immunology teaches. So, what happened later in the year to alter the clearly held view of SAGE that the virus would manifest itself in a single wave? We need SAGE to tell us.
PCR is a powerful tool, but has weaknesses when used on an industrial scale
Despite this bothersome oddity about a ‘second wave’ and almost as if there was a plan for one, the PCR (polymerase chain reaction) testing infrastructure in the UK began to be reshaped.
PCR is a quite remarkable technique, which has unparalleled ability to find truly tiny quantities of a fragment of a genetic sequence, right down to the level of finding a single, broken fragment of a virus in a messy biological sample. There are notable limitations, well known to those who’ve personally used PCR in a research context. The most important one is its propensity to suffer from contamination, and the integrity of a PCR is very easily destroyed by invisible levels of contamination even in the hands of an expert, working alone and on a small handful of samples.
This is a good moment to mention that the PCR test protocol for SARS-CoV-2, which everyone in the world is now using, was invented in the lab of Prof Drosten in Berlin. The scientific paper in which the method was described was published in January 2020, two days after the manuscript was submitted. One of the authors of the paper is on the editorial board of the journal that published it. There is concern that this extremely important article, which contains a PCR test protocol that has been used to run hundreds of millions of PCR tests across the world, including the UK, was not peer-reviewed. No peer review report has been released, despite many requests to do so. Furthermore, as a method, it contains numerous technical weaknesses, some of which are serious and highly complex. Suffice to say that a very detailed dissection of the paper and of the Drosten protocol has been made by Drs Borger and Malhotra, experienced and concerned molecular biologists. A group of other medics and scientists (of which I am one) have put their names to a letter, which accompanies the dissection, to the whole editorial board of the journal, Eurosurveillance, demanding that the paper be retracted. This was submitted on Nov 26th.
In addition, the Portuguese high court determined two weeks ago that this PCR test is not a reliable way to determine the health status or infectiousness of citizens, nor to restrain their movements. Other countries are also receiving legal challenges, one being submitted earlier this week in Germany by Reiner Fuellmich, a lawyer who successfully sued VW in relation to diesel emissions (The YouTube video in which Fuellmich sets out the principal points of concern about the misuse of PCR has been removed). I am aware of other legal challenges being assembled in further countries, including Italy, Switzerland and South Africa. With the scientific validity of this test under severe challenges, I believe it must immediately be withdrawn from use.
There are deep concerns internationally about the reliability and selectivity of this PCR test protocol and this should be borne in mind through the rest of this article.
NHS labs ran PCR competently in spring
In spring, the relatively constrained amount of PCR testing was at least conducted independently by very many, experienced labs and I am of the view that it was trustworthy, reaching more than adequate numbers of tests by the end of May (50k per day). Now it’s being run in newly-established large, private labs and most of their current staff are far less experienced than those in the NHS labs. We have no idea why this has happened. Regardless of any concerns about testing capacity, the need was and should have been expected only to be of limited duration. Remember, viruses don’t do waves and we’d already been fully exposed to the virus. Of course, it was argued that “a second wave was coming”, so we’d need more capacity. But as I’ve already shown, the certainty of expectation of a ‘second wave’ was bizarre and unaccountable.
So why was PCR testing removed from NHS labs? One answer is because they didn’t have the capacity to cope with testing requirements for a ‘second wave’. But this is circular: it was simply impossible to claim with certainty that there’d be such a wave. Also, it’s not true that the NHS labs couldn’t cope. As a staff member there pointed out: “I want to know why the new super-labs have been set up, because if they gave the NHS labs the (consumables) resources they could easily do the tests. Our lab has been ready for ages to do large numbers of tests. We have the equipment and we have staff. We lack only the test kits and these are not available to any new labs, either.”
It wasn’t just NHS lab staff who were perturbed by the move. I’m quoting extensively from this article because it contains crucial information. The President of the Institute of Biomedical Sciences (IBMS), the leading professional body in the field of biomedical science, said:
It concerns me when I see significant investments being made in mass testing centres that are planning to conduct 75,000 of the 100,000 tests a day. These facilities would be a welcome resource and take pressure off the NHS if the issue around testing was one of capacity. However, we are clear that it is a global supply shortage holding biomedical scientists back, not a lack of capacity. The profession is now rightly concerned that introducing these mass testing centres may only serve to increase competition for what are already scarce supplies and that NHS testing numbers will fall if their laboratories are competing with the testing centres for COVID-19 testing kits and reagents in a ‘Wild West testing’ scenario. The UK must avoid this for the sake of patient safety. It is clear that two testing streams now exist: one delivered by highly qualified and experienced Health and Care Professions Council (HCPC) registered biomedical scientists working in heavily regulated United Kingdom Accreditation Services (UKAS) accredited laboratories, the other delivered mainly by volunteer unregistered staff in unaccredited laboratories that have been established within a few weeks. This has presented another key concern – in that we have not been involved in assuring the quality of the testing centres and are now being kept at arm’s length from their processes, even when they exist close to large NHS laboratories.
On proof reading this article, I was struck at how powerful the case was for keeping things under the quality control of the NHS. What could the motives against this sensible plan have possibly been?
These testing facilities were presumably expected to be temporary. If so, why would it make sense to spend large sums of money and to displace equipment and consumables, which were the sole key missing item when the Lighthouse super-labs were announced, instead of using existing, keen, accredited staff who knew what they were doing? Those new labs would be as limited by consumables as the NHS labs.
We never really needed mass testing of those without symptoms
Arguably, we would never have been short on capacity if we had limited the testing to those with symptoms. The only reason one might even consider mass testing of those without symptoms is if you were convinced that those without symptoms were significant sources of transmission. This has always seemed to me to be a very tenuous assumption. Specifically, respiratory viruses are spread by droplets of secretions and generally the expulsion of these is linked to the symptoms of infection – coughing in particular. Humans have evolved over millions of years to recognise threats to health by close observation of the health status of others. It works well. We’re familiar with avoiding those with flu-like symptoms in winter and behaving responsibly by staying away from work and vulnerable people when we are symptomatic. The burden of proof rests with those claiming something very different in the case of SARS-CoV-2 to show conclusively that asymptomatic people are indeed major sources of transmission. I don’t think that case has at all been made. The medical literature on this is contradictory but almost all the papers claiming such transmission originated in China.
Consequently, there is simply no need to get into the business of mass testing the population. Indeed, as we will see, such mass testing brings with it, when using PCR as the method, a severe risk of what we call a “PCR false positive pseudo-epidemic”. This could never happen if we were not using PCR mass testing of the mostly well. So, for whatever reason and against all historical precedent and immunological reasoning, a major initiative was launched with the goal of reaching 500,000 tests a day by year’s end. Again, unaccountably, the Government didn’t just get on and build these new labs, working in parallel with the available NHS capabilities. Instead, responsibility for testing was swept out from 44 NHS labs, with skilled and accredited staff who’d already been running SARS-CoV-2 PCR. In their place, new labs were created, outside the help and control network of the Institute of Biomedical Sciences. These Lighthouse Labs are still not all fully accredited under UKAS to ISO 15189, a quality management system accreditation relating to medical laboratories.
There is a reliable test, fully-characterised and already validated with real-world use
At the end of October, the British Army was called in to help Liverpool City Council find the cases which the ONS PCR testing survey predicted should be there but which were no longer being found in the numbers expected. It was possible that people were no longer coming forward to be tested, though there is no way to be sure of this. Despite not having sought consent from the parents of school children and the absence before the survey began of proper protocols and ethics review, scores of thousands of people were tested using a lateral-flow test (LFT). (See here and here for more details on the LFT.) These look rather like the familiar pregnancy test kits you can purchase over the counter. They look similar, because they use related tried and trusted technology to detect virus proteins in the swab, not RNA. All tests have limits and weaknesses. However, the LFTs are not subject to the same flaws as PCR – specifically the risk of over-amplification and of cross-contamination before the test is actually run. LFT has similar sensitivity and specificity in the lab to PCR. It is certainly capable of identifying the same proportion of those truly infected as PCR.
In brief, the army found very few people with positive LFT results, only slightly higher than the background operational false positive rate: just over 0.3%, values expected when the tests are used in the real world. Since testing began, the positive rate has tended to a mean of 0.7% which might mean a few people were positive. My own experience of reading around this area is that this (around 0.7%) is almost certainly the true false positive rate when, in the real-world, careful but inexpert people administer the LFT. It meant that, in the city in the centre of the national hotspot for COVID-19, almost no one had the virus. This experiment has been repeated for 8,000 people in Merthyr Tydfil resulting in 0.77% testing positive. That these two test series have returned such similar values suggests that this is indeed the true, operational false positive rate for the LFT, though another test series will be helpful in refining that possible interpretation. Some leapt to criticise the LFT, as if it was its fault that it couldn’t find the expected cases. Of course, to many of us, the results were exactly what we’d expected, because we were by then sure that PCR was wildly over-reading. PCR has gone wrong before and Occam’s razor indicated that this was by far the most likely explanation for the otherwise inexplicable failure of PCR “cases” to correlate with symptomatic disease. These are the kind of results expected in populations protected by herd immunity. They’re completely inconsistent with a city and town in the grip of a highly-infectious respiratory virus.
To the Lighthouse
By September, the great bulk of PCR testing was being run by large, private labs, some of which are called Lighthouse Labs, and I’ll use this term as a coverall for all such labs. It was as September began that literally incredible things started to happen. Students returning to University towns were all required to submit to swabbing and PCR testing. We were then told there was an epidemic running through young people and it was just a matter of time before it reached the elderly and that would be that. The percentage of tests which were returning positive started skyrocketing, reaching in some towns values that were close to those in A&E at the peak of the pandemic in April. Strong linkage was observed between numbers of tests run and their positivity. This is most odd and can happen if the error rate increases with the pressure on the testing system.
Now, in late November, we are told there are sometimes 25,000 new “cases” daily and that several hundred daily “COVID-19 deaths” are occurring. How can this be happening if I’m right and the population has achieved herd immunity (as supported by large numbers of scientific papers detailing extensive T-cell immunity, as well as careful examination of the profile of deaths in spring vs recently, and the examination of patterns of deaths around the country recently as compared with spring)? It’s a conundrum.
As the numbers of daily PCR tests conducted began to climb very steeply, reaching 370,000 per day in mid-November, many of us have had the uncomfortable feeling that the chances of PCR testing on this scale returning accurate results are vanishingly small. To avoid cross-contamination and to have such high throughput flies in the face of decades of relevant experience for some of us. The classic triad of speed, throughput and quality always has one of them as the lead, limiting factor. In this case, my entire career experience tells me that the limiting factor is quality.
How we can square these claims of tens of thousands of daily “cases” and an unprecedented ‘second wave’ of deaths with the unfeasible quantity of testing using a technique considered by bench experts difficult to perform reliably even on a small scale?
A PCR false positive pseudo-epidemic looks just like a real epidemic, but isn’t
It’s important to appreciate while digesting this counter-narrative which, unlike the official line, is at least internally consistent, that the only data suggesting a ‘second wave’ is upon us are PCR results. Everything is dependent on this. A “case” is a positive PCR test. No symptoms are involved. A “COVID-19 admission” to a hospital is a person testing positive by PCR before, on entry or at any time during a hospital stay, no matter the reason for the admission or the symptoms the patient is presenting. A “COVID-19 death” is any death within 28 days of a positive PCR test. If there is any doubt about the reliability of the PCR test, all of this falls away at a single stroke.
I have to tell you that there is more than common-or-garden doubt about the PCR mass testing that purports to identify the virus. We have very strong evidence that the PCR mass testing as currently conducted is completely worthless.
At this point, it’s appropriate to give the game away and invite you to read the explanation that the team of which I’m part have assembled.
In brief: the pandemic was over by June and herd immunity was the main force which turned the pandemic and pressed it into retreat. In the autumn, the claimed “cases” are an artefact of a deranged testing system, which I explain in detail below. While there is some COVID-19 along the lines of the “secondary ripple” concept explained above, it has occurred primarily in regions, cities and districts that were less hard hit in the spring. Real COVID-19 is self-limiting and may already have peaked in some Northern towns. It will not return in force, and the example again is London. Even here, certain boroughs, e.g. Camden and Sutton, have had minimal positive test results. I’ve explained a number of times how this happened – the prominent role of prior immunity is often ignored or misunderstood. The extent of this was so large that, coupled with the uneven spread of infection, it needed only a low percentage of the population to be infected before herd immunity was reached.
That’s it. All the rest is a PCR false positive pseudo-epidemic. The cure, of course, as it has been in the past when PCR has replaced the pandemic itself as the menace in the land, is to stop PCR mass testing.
In case you’re still not convinced and think several hundred people are dying of COVID-19 each day, please watch this 10 min explainer video, created by data scientist Joel Smalley. By the end you will appreciate how the difference between reporting date and date of occurrence in relation to deaths and the large difference in this regard between COVID-19 deaths, most of which occur in hospital, and non-COVID-19 deaths, many of which happen at home, gives at any moment an impression of excess deaths which, when corrected for this differential delay, collapses into nothing or into such a small signal that surely it’s not faintly a public health concern. It’s also important to be aware that, for the best of intentions, physicians are too quick to assign COVID-19 as the cause of death, partly because the death sometimes has the right kind of elements, but mostly because the rules require them to: any death within 28 days of a positive test has to be recorded as a COVID-19 death, no matter what the circumstances. The degree of misattribution is so large that the number of deaths from the top 10 leading causes have been pushed far below normal levels, which is highly suggestive of these deaths having been mislabelled. Do note, you should at this point expect some excess deaths, if from nothing else, a number of people dying – mostly at home – from non-COVID-19 causes, a result of restricted access to healthcare for eight months.
I think the evidence is unequivocal that we are in a PCR false positive pseudo-epidemic
It’s happened before, with whooping cough (caused by a bacterium, but the technique for diagnosing the disease was the same, PCR). Hundreds of apparent “cases” were diagnosed at a hospital in New Hampshire using PCR and physicians fitted the symptoms of various coughs and colds to what the “gold standard test” was telling them. In fact, not a single person had the disease. The positivity in the PCR test was around 15%, but no actual infection was found. 100% of the PCR positives were false. Unrealistically high positivity and no recent, independent confirmation of infection is now the situation in UK.
To the Lighthouse (again)
How can this PCR false positive pseudo-epidemic be occurring? A false positive is simply a positive outcome of a test when the item sought was absent from the original sample (there are a variety of sources of false positives and they are often ignored or confused: https://logicinthetimeofcovid.com/2020/11/28/a-miscarriage-of-diagn...). Most false positives in PCR occur due to cross-contamination. This can occur if a sample containing the virus is even briefly in contact with a sample not containing the virus. Contamination can and does happen at any of the stages from sample acquisition all the way into the reaction vessel in which the cyclical amplification of PCR takes place. This contamination can include the reference material used to confirm the test run is working, the so-called positive control, itself a piece of synthetic viral RNA. Such positive controls are potent sources of error as they are an intensely concentrated supply of the very material sought in miniscule amounts by the test, right down to a single, broken fragment of virus. Other common sources of contamination are a small number of samples which actually do contain the virus, which almost certainly continues to circulate at low levels and may already have become endemic (like the four, common cold-inducing coronaviruses, OC43, HKU1, 229E and NL63).
It is my opinion, and I am not alone, that industrialized molecular biology PCR mass testing is and always was unfeasible on the scale it’s currently being conducted. With high speed and throughput, something has to give and in this case it’s quality. Here are just a few of the reasons why you should no longer have any faith or confidence in the PCR testing in use in UK. As the drive to industrialize the process proceeded, responsibility for PCR testing was mostly moved into one centralised set of facilities called Lighthouse Labs. I shall describe testimony (for Milton Keynes) and video evidence (Randox in Northern Ireland) which are concordant.
We have horrifyingly clear evidence that the work processes, staffing, lack of quality control and external validation means that this facility cannot work reliably and produce trustworthy testing results. I have spoken at length to the brave scientist who’s blown the whistle on the Milton Keynes super-lab, Dr Julian Harris, who is one of the most experienced lab PCR scientists in the UK. He was been involved in high biosecurity level labs since 1987 and has operated PCR for decades. What’s been missed in the expose is that his concerns are not only with health and safety (though these are important). It is that in his long experience it’s literally not possible for a facility like the building in Milton Keynes to enable conduct of sample preparation and PCR mass testing without frequent, persistent and intractable cross-contamination. The effect of this is to greatly increase the number of “positive” tests.
No-one competent is inspecting these facilities, staff processes and results. The only person capable of looking from stern to stem who’s actually done so is Dr Julian Harris and he unequivocally condemns the operation. He highlighted overcrowded, biosecure workspaces, the absence of health and safety training, poor safety protocols and hand-washing facilities and a lack of suitable PPE. The Health and Safety Executive was called in (by Dr Harris). Management of the facility failed to answer requests to set up a visit, so eventually, they made unannounced visits in late-September (see letters from the HSE at the base of Dr Harris’s piece). Their visits, which most unusually (and tells us of the degree of concern they felt) were accompanied by HM Inspector of Health and Safety, uncovered safety breaches at the Lighthouse Lab in Milton Keynes.
“I found they’ve got no experience with this sort of facility or handling bio-hazardous materials, and then they’re just launched into this activity,” Dr Harris says of the Milton Keynes team. Dr Harris was so troubled by what he saw that he contacted the Health and Safety Executive (HSE). He saw two people using biosecurity cabinets – enclosed, ventilated workspaces where scientists open the tubes containing the contaminated swabs – which were only calibrated to have protective airflow for one person. “Once you disrupt that [airflow], you might as well be working on an open bench. It just disrupts the whole reason for a cabinet to protect the operator. And it is really disturbing,” Dr Harris says. He alleges that the lab recruited local young people to work long shifts.
Dr Harris says he saw mobile phones being used in the labs and then taken to the canteen. The HSE visited the Milton Keynes lab and found five material breaches of health and safety legislation. The manager admitted that the training in place did not look “robust enough” for these new recruits. Dr Harris tells me that there was little or no H and S training at all, despite the facility being rated BSL2.
It’s not only procedural issues in the labs that are concerning. With individual PCR tests, the scientist views the change in signal vs cycle and determines whether a test is positive, negative or indeterminate. In high throughput mode, this can only be done by software. Thus, the choice of provider is absolutely crucial to the accuracy and trustworthiness of the output, not only for an individual sample but also at a population level. For reasons not explained, the facility chose a software product which was apparently inferior.... Why did the Lighthouse Lab choose an inferior product? In the example given, it ‘under-called’ positives but that doesn’t tell you that’s what it does now. What it does tell us is that it’s less reliable at ‘calling’ results. Surely the firm whose product performed better and had already passed regulatory standards would have been the better choice?
Underscoring their problems with staffing, the Lighthouse Lab did have a quality management system (QMS) specialist while Dr Harris worked there. However, that person resigned and, as far as I know, has not yet been replaced with someone of equivalent experience. This will undoubtedly have contributed to continuing failure to be UKAS accredited to ISO 15189, quality and competence in medical laboratories. While this can be seen as voluntary, the customer (Her Majesty’s Government) determines whether or not such accreditation is essential. Given there has never been a medical diagnostic test of such importance in the entire history of the nation, HMG must surely have specified ISO 15189 accreditation. If they have not, that is in my view a severe dereliction of duty. In any case, its absence does not in any way reduce the need to run these critical PCR tests to the highest standards and for the output to be trustworthy.
Separately, though the HSE accreditation doesn’t prove quality and accuracy of the end product, the test results, and that the facility is still not so accredited, indicates a continuing failure to get to grips with the overlapping issues in the lab which directly pertain to end-to-end sample integrity.
This detailed recounting of evidence is not designed to be a teach-in on health and safety, important though that is. It is instead to demonstrate that neither management nor staff have the scrupulous attention to every detail required to ensure sample integrity from end-to-end, which is merely the starting point to have any chance at all to successfully run this delicate and powerful technique, which is notoriously susceptible to cross-contamination of the smallest kind. The act of touching the base of the flow hood with a gloved hand, if there is the smallest drop of medium which might contain virus, is sufficient to convert negative tubes handled afterwards into positives.
For every one of the scores of thousands of tests per day to be conducted, each swab bag must be opened, the tube lids removed and some medium pipetted out. This requires the careful use of highly engineered micropipettes. Many such tubes were routinely observed by Dr Harris to be taken into the flow hood at one time, and some of the tubes leak, potentially contaminating the outside and anything they touch. These preparative steps are all performed manually, by staff with little to no PCR experience and in many cases, no experience of professional laboratory work at all. As a hallmark of how low the hiring bar has been set, the Milton Keynes facility has a staff member who carries out ‘pipette training’. This is a fundamental skill usually learnt at the beginning of a scientific career. I’ve never heard of such a role anywhere before in 39 years of conducting and supervising laboratory work in UK.
Finally, I asked Dr Harris when, in the sequence of steps, the ‘negative control’ samples were placed. The most vulnerable part of the task to cross-contamination is the bag opening to sample placement in the final, racked tubes, which are then placed into the automated workflow, finally dispensing sample for testing into the PCR plate. Therefore, I expected to be told that there were several negative controls. One should be to insert some unused tubes (with their own bar codes) early on, so that, if there was cross-contamination, it would be detected in the final, PCR step.
But no. The sole, negative control is virus-free medium, carefully placed into the final unused well in the 96-well plate in which the actual PCR step is conducted. This bypasses all the cross-contamination steps and means any cross-contamination can never be detected. That’s not only bad scientific technique but, in my view, tantamount to a cover-up. If I was teaching an undergraduate student, and they came up with this as an experimental design, I would fail them. It’s no wonder that the positivity rate – the percentage of tests which come up positive – is so high as to be literally unbelievable. I’m sure the Lighthouse Lab tells its client that there’s no evidence of cross-contamination, as the negative controls are consistently free of virus. Yet we drive our entire national policy on the strength of this?
Randox
There are a small group of large labs which were set up at speed to become “Lighthouse Labs” or “Superlabs”. A second one, the Randox facility in Antrim, Northern Ireland, has been the subject of a Channel 4 Dispatches program. This detailed documentary film centres on this very large, private contract lab testing over 100K COVID-19 samples per day using PCR. Watching this program with an eye of someone experienced in lab procedures related to mass testing (though not this technique) I observed: workers cutting open plastic bags containing swab samples in tubes, some of which had leaked. The scissors were then used to open the next bag and so on. Tubes were wiped externally using a wipe, but the same wipe was used to mop the outsides of several tubes in a row. The tubes were then placed on their sides in a tray, where they were free to roll around and touch other tubes. Workers kept on the same pair of disposable gloves while opening a large number of such bags, one after another. A worker commented that just under 10% of tubes with red caps leaked. Randox stated that it didn’t make the tubes and that a fix was in progress.
A consultant microbiologist, who’d run an NHS pathology lab for 1- years, commented for the film: “If you have a tube which has leaked and is in your unpacking environment, it’s then quite easy for that to get onto other tubes. If the leaked sample was positive, it would cause the other tubes to become positive. These are very sensitive tests we’re using and it’s very easy to get (contamination-related) false positives. We would be shut down if we performed that way”.
Taking Milton Keynes and Randox together, I contend that there was a policy decision to create an expectation in the minds of most people that a ‘second wave’ was expected, and that this would require increased testing capability. The conditions which resulted from these industrialisation attempts (Lighthouse Labs and similar) by virtue of the poor sample handling evidenced in two examples (Milton Keynes, in the same building which houses the U.K. Biobank, and Randox, on a former military base) actively created that ‘second wave’ (of misdiagnosed cases, admissions and deaths). I believe the unavoidable conclusion is that the mechanism whereby large numbers of “cases” were and still are being created is insidious, uncontrolled and undetected cross-contamination during the swab sample processing stages.
I have no doubt that those conducting the manual steps of pipetting are doing their best. But they do not have the skills and experience of this technique, which must be performed repetitively and for hours, while never creating a burst of micro-aerosol as they drive the thumb plunger on the pipette slightly too fast, or creating a micro-splash as they change the disposable tip. They must never contaminate a fingertip of a glove as they open a potentially leaking tube and then touch another. They must never disturb the laminar airflow in the hoods so as to facilitate invisible levels of contamination from one tube to another. There are so many ways in which miniature levels of contamination compromise sample integrity and increase the number of positives, and no one has taught them to avoid them all.
In these two PCR mass testing factories, among the largest, there is now strong evidence of completely inadequate effort to ensure that end-to-end sample integrity is maintained. These are, in my view, simulacra of proper testing facilities. Meanwhile, daily testing capacity has grown considerably, approaching the goal of conducting 500,000 tests by PCR daily.
Criticisms of PCR (again)
Even if the Lighthouse Labs did work from a technical perspective, the Government has admitted that PCR’s characteristics as a test are literally out of control. Lord Bethel confirmed in a written answer that the UK Government does not know the operational false positive rate (OFPR). While the Government claimed it could adopt as an estimate a range from prior related tests (0.8-2.3%) this is tendentious. These earlier tests were done by highly experienced lab scientists working at relatively small scale. Each PCR test will have a unique false positive rate dependant on the design of the test and it cannot be deduced from other tests. The Lighthouse Labs are mostly staffed by young and inexperienced people, many of whom have never previously worked professionally in a lab. It is absurd to suggest the combination of inexperienced staff, coupled with an industrialized process of a technique so sensitive to cross-contamination that such cross-contamination is a routine problem in research labs performed by careful, knowledgeable scientists, could yield reliable, trustworthy results.
I maintain that lack of knowledge of the OFPR alone renders this PCR test in this configuration completely incapable of providing trustworthy results. If this was a diagnostic test in use in the NHS today, no physician would submit a patient sample to it, because it would be impossible to interpret a positive result. Of course, it is a diagnostic test in use today.
In summary, I argue that it is criminally dangerous to drive policy based in any way on this test (set up the way it is) and its results. No amount of argument or prevarication can alter these damning facts.
Conclusions
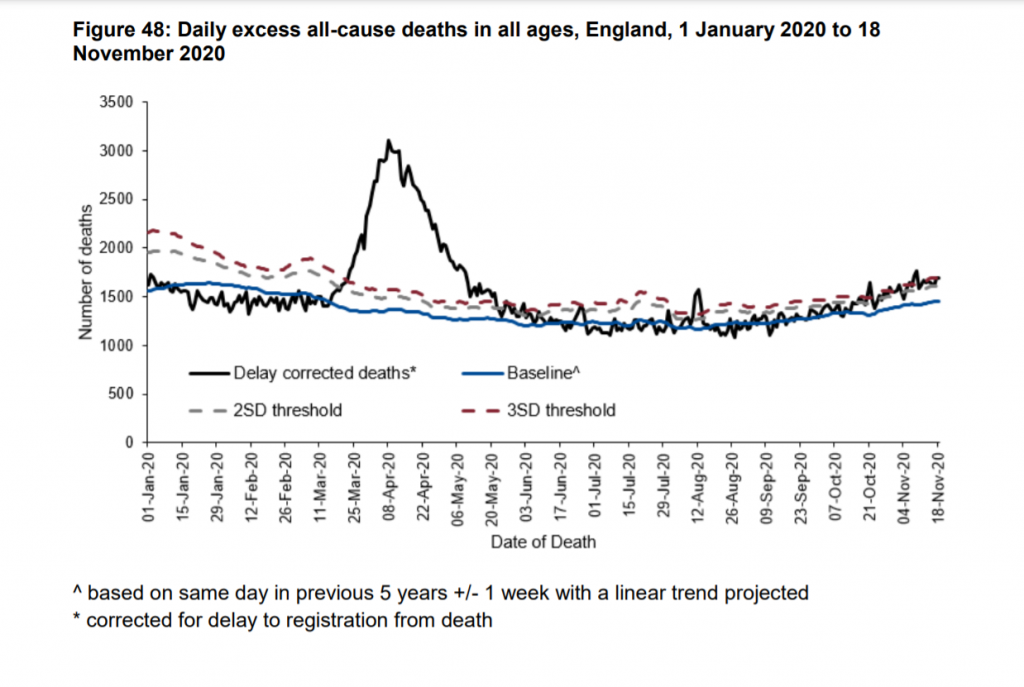
Source: Public Health England weekly national Influenza and COVID- 19 surveillance report, Week 48 (w/e Nov 26th)
The entire ‘second wave’ is supported solely on the back of a flawed mass PCR test, which at industrialized scale was never, in my view and the views of others skilled in PCR, capable of delivering trustworthy results. I have detailed the evidence supporting the claim that the autumn PCR test results are not reliably detecting COVID-19 infection. It may seem a leap to damn the PCR test and claim that there isn’t an epidemic but a pseudo-epidemic. But even in the hands of skilled and careful people, the strange phenomenon of the PCR false positive pseudo-epidemic has occurred several times before. In large, industrialised labs, it is very likely that significant and unmeasured cross-contamination related false positive rates are occurring.
The key sign of a PCR false positive pseudo-epidemic is the relative paucity of excess deaths equal to the deaths claimed to be occurring as a result of the lethal infective agent. This key sign is present.
The unprecedented “’second wave’ conundrum is solved. It’s of course not happening, but why a ‘second wave’ was talked up, months before unreliable PCR testing data was brought into service, demands deeper investigation. It’s not a science matter: not unless the team predicting the wave can produce the scientific literature upon which the prediction and modelling was based.
As a reference, I spent over an hour consulting with the owner-manager of a well-run facility in another country, which mainly serves private clients. This person only hires staff to do this kind of work who have at least four years’ experience of PCR, not just of highly competent laboratory experience. These will in almost all cases be post-doctoral students, having already obtained a research-based PhD involving use of PCR techniques.
Those who observe that PCR testing at scale elsewhere seems to run well tell us only that it can be done acceptably if it’s set up carefully. That’s assuming you can trust their results, something to which my research cannot extend. In any case, in no way does that observation undermine any of what I’ve written.
Until we end the use of PCR mass testing, there is no chance that “cases” will reduce to very low levels. Lateral flow tests must become the gold standard test for COVID with PCR only used for confirmatory diagnosis. This will minimise the number of PCR tests that need to be performed allowing testing to return to competent NHS laboratories. Without such an intervention, even if the virus stopped circulating, I believe we’ll still hear of tens of thousands of “cases” every day, and several hundred deaths.
As the above graph clearly shows, there was a notable peak of excess deaths due to SARS-CoV-2 in the spring, but it has not returned. As noted earlier, some excess deaths are now to be expected at very least as a consequence of prolonged and widespread restricted access to the NHS.
So, just one wave, as expected. The ‘secondwave’ of “cases” and even “COVID-19 deaths” are an artefact of flawed testing.
Source: https://lockdownsceptics.org

You need to be a member of Saviors Of Earth to add comments!
Join Saviors Of Earth